

Operative Morbidity and Mortality of Aortic Stenosis with Left Ventricular Dysfunction
Clinical Medicine And Health Research Journal,
Vol. 4 No. 2 (2024),
28 April 2024
,
Page 887-892
https://doi.org/10.18535/cmhrj.v4i2.352
Abstract
Objectives: Study of the operative morbidity and mortality of aortic stenosis with left ventricular systolic dysfunction (LVEF < or = 35%).
Method: 73 patients with a mean age of 55+/-8 years, 59 of whom were men, underwent surgery between January 2014 and december 2019; 14% (10/73) of these patients had a pre-operative low trans-valvular aortic gradient (<30mmHg).
We determined the factors predictive of operative mortality using univariate and multivariate analyses, analysed changes in functional status and left ventricular ejection fraction, and compared operative mortality and late survival in these 73 patients with those in a control group with no left ventricular dysfunction.
Results: The mean NYHA stage, before and after aortic valve replacement, fell from 3.8 to 1.7, and the mean improvement in LVEF was 28+/-13.
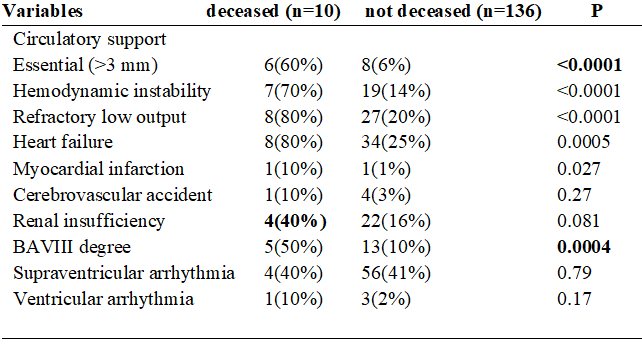
In univariate analysis, the parameters significantly associated with operative mortality were arterial hypertension (p=0.039), congestive heart failure (p=0.030), a smaller indexed left ventricular mass (p=0.039), a mean gradient of less than 30mmHg (at the limit of significance (p=0.053)), a low cardiac index (p=0.0045), and mono-truncular coronary involvement (p=0.042).
In multivariate analysis, no variable was identified as an independent predictor of operative mortality.
Conclusion: Operative mortality was significantly higher 11.7%vs 2.9% (p=0.048) in the group with left ventricular dysfunction, although late survival rates were similar in the 2 groups (86.8% vs 93%).
Given the spontaneous prognosis and the increased operative risk, these patients should be operated on.
- aortic stenosis, LV dysfunction, surgery, mortality
How to Cite
Download Citation
References
- Article Viewed: 0 Total Download
##plugins.themes.ojsPlusA.frontend.article.downloadstatastics##
Cover Image
